Renal Artery Denervation for High Blood Pressure
About High Blood Pressure (Hypertension)?
What is hypertension?
High blood pressure, known as hypertension, is an important worldwide issue that affects nearly a billion of the world’s population. At any one time it is estimated that 25% of the UK have hypertension. The disorder becomes more common with advancing age. Patients with hypertension are at an increased risk of cardiovascular disease such as stroke, heart attack, heart failure, kidney problems and eye problems. However, a small reduction in blood pressure can significantly reduce the risk of cardiovascular disease (Including stroke and heart attack). A vast majority of patients have 'Essential hypertension', which is the main cause of high blood pressure and is treated as described below, this can often be done in the first place by Cardiologists but more specialised cases need to be sent to an accredited hypertension specialist. A small proportion of patients have hypertension due to other causes, such as kidney disease, this is known as 'Secondary hypertension'. Treatment of 'Secondary hypertension' is not covered here and usually done by an accredited Hypertension specialist (see below).
What is the treatment for hypertension?
The most important treatment for hypertension is a change in lifestyle factors such as: increased physical activity, weight loss, more healthy diet (including reduced salt intake) and a reduction in alcohol intake. However, despite lifestyle measures taking medication designed to lower your blood pressure (known as anti-hypertensive drugs) is usually necessary. It does not matter how many medications you take as long as your blood pressure is safely controlled. It is common for people to take more than one drug to control their blood pressure, in addition to lifestyle changes.
What is treatment-resistant hypertension?
Treatment-resistant hypertension is defined as blood pressure that remains high in spite of compliance with full doses of three or more antihypertensive medications of different classes; ideally, one of the three agents should be a diuretic and the treatment plan must include attention to lifestyle measures. Data from small clinical studies and observational cohorts show that patients with resistant hypertension have approximately a three-fold increased risk for cardiovascular events compared with that of patients with controlled hypertension. The proportion of patients with treatment resistant hypertension is estimated to be 5-10% of those with hypertension.
Anyone with hypertension that is difficult to treat should see an accredited specialist in hypertension first, who may organise further specialist tests first and advise on optimising drug treatment. Although none of the Cardiologists at Wessex Cardiology are accredited Hypertension specialists, we can treat simple cases. Then, if an accredited specialist hypertension opinion is needed, we can refer you to an accredited hypertension colleague who runs a specialist hypertension clinic at the Spire Southampton Hospital.
Currently specialist procedures for hypertension, such as renal denervation (see below) are only available in clinical trials in the UK.
High blood pressure, known as hypertension, is an important worldwide issue that affects nearly a billion of the world’s population. At any one time it is estimated that 25% of the UK have hypertension. The disorder becomes more common with advancing age. Patients with hypertension are at an increased risk of cardiovascular disease such as stroke, heart attack, heart failure, kidney problems and eye problems. However, a small reduction in blood pressure can significantly reduce the risk of cardiovascular disease (Including stroke and heart attack). A vast majority of patients have 'Essential hypertension', which is the main cause of high blood pressure and is treated as described below, this can often be done in the first place by Cardiologists but more specialised cases need to be sent to an accredited hypertension specialist. A small proportion of patients have hypertension due to other causes, such as kidney disease, this is known as 'Secondary hypertension'. Treatment of 'Secondary hypertension' is not covered here and usually done by an accredited Hypertension specialist (see below).
What is the treatment for hypertension?
The most important treatment for hypertension is a change in lifestyle factors such as: increased physical activity, weight loss, more healthy diet (including reduced salt intake) and a reduction in alcohol intake. However, despite lifestyle measures taking medication designed to lower your blood pressure (known as anti-hypertensive drugs) is usually necessary. It does not matter how many medications you take as long as your blood pressure is safely controlled. It is common for people to take more than one drug to control their blood pressure, in addition to lifestyle changes.
What is treatment-resistant hypertension?
Treatment-resistant hypertension is defined as blood pressure that remains high in spite of compliance with full doses of three or more antihypertensive medications of different classes; ideally, one of the three agents should be a diuretic and the treatment plan must include attention to lifestyle measures. Data from small clinical studies and observational cohorts show that patients with resistant hypertension have approximately a three-fold increased risk for cardiovascular events compared with that of patients with controlled hypertension. The proportion of patients with treatment resistant hypertension is estimated to be 5-10% of those with hypertension.
Anyone with hypertension that is difficult to treat should see an accredited specialist in hypertension first, who may organise further specialist tests first and advise on optimising drug treatment. Although none of the Cardiologists at Wessex Cardiology are accredited Hypertension specialists, we can treat simple cases. Then, if an accredited specialist hypertension opinion is needed, we can refer you to an accredited hypertension colleague who runs a specialist hypertension clinic at the Spire Southampton Hospital.
Currently specialist procedures for hypertension, such as renal denervation (see below) are only available in clinical trials in the UK.
About renal denervation
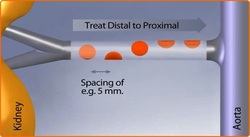
Renal artery denervation (RDN) is a new treatment for patients that have treatment-resistant essential hypertension. This involves a thin steerable catheter that is inserted via an artery in the groin and positioned to the renal nerves along the renal arteries supplying both kidneys. This catheter delivers radiofrequency energy in a series of two minute ablations along each renal artery to disrupt the nerves. Deactivation of these nerves should suppress excess sympathetic nerve drive, which contributes to high blood pressure, and therefore reduce your blood pressure. The procedure should take 40 minutes and will require an overnight stay, as you are given a lot of medicine to make you sleepy during the procedure and prevent reduce pain.
A clinical trial published in the Lancet, 2010 showed an average reduction of 32/12mm Hg in blood pressure. There have been no serious complications to date related to any of the patients treated with renal artery denervation. These early trials indicate that renal artery denervation is both an effective and safe treatment for patients with treatment-resistant hypertension. Recent 2 year follow up data shows a sustained treatment effect from this procedure. More than 4000 patients have been treated worldwide with this procedure.
Consultant Interventional Cardiologists Dr Wilkinson and Dr Simpson set up a renal denervation programme at Southampton General Hospital in 2012, in conjunction with a multi-disciplinary team. Dr Wilkinson did the first six cases at Southampton General Hospital (see media below) in conjunction with Dr Allan Odurny, a consultant Interventional Radiologist and went on to do a number of cases before funding was suspended. The NHS was due to commission this procedure in 2014, however following publication of more research it was decided not to commission this procedure and it is only available in clinical trials presently. These will hopefully provide more robust evidence to allow commissioning of this procedure in the future.
A clinical trial published in the Lancet, 2010 showed an average reduction of 32/12mm Hg in blood pressure. There have been no serious complications to date related to any of the patients treated with renal artery denervation. These early trials indicate that renal artery denervation is both an effective and safe treatment for patients with treatment-resistant hypertension. Recent 2 year follow up data shows a sustained treatment effect from this procedure. More than 4000 patients have been treated worldwide with this procedure.
Consultant Interventional Cardiologists Dr Wilkinson and Dr Simpson set up a renal denervation programme at Southampton General Hospital in 2012, in conjunction with a multi-disciplinary team. Dr Wilkinson did the first six cases at Southampton General Hospital (see media below) in conjunction with Dr Allan Odurny, a consultant Interventional Radiologist and went on to do a number of cases before funding was suspended. The NHS was due to commission this procedure in 2014, however following publication of more research it was decided not to commission this procedure and it is only available in clinical trials presently. These will hopefully provide more robust evidence to allow commissioning of this procedure in the future.
What to expect if I have this procedure?
What happens before my procedure?
All patients will be assessed for suitability for this treatment and will need to undergo the following work-up prior to any treatment:
· A full consultation, including a full physical examination
· Evaluate Blood Pressure (BP) three times in clinic
· Have 24 hour ambulatory blood pressure monitor to demonstrate high blood pressure despite optimal treatment
· Evaluate kidney (renal) function
· Screen for diabetes
· Screen for other conditions that may prohibit renal denervation such as recent MI, pregnancy, etc. (Holter ECG, ambulatory BP monitoring, echocardiogram, cardiac MRI, NT-proBNP, etc.)
· Perform renal artery imaging with MRI scan
Once this work-up has been completed by a hypertension specialist, you may then be eligible for renal artery denervation. If you have secondary causes of hypertension, kidney failure or unsuitable renal arteries (assessed on MRI) then you cannot have the procedure. Your suitability for the procedure will be decided at a specialist MDT.
What happens after my procedure?
Following the procedure the following tests will be performed:
· Conduct a further physical examination
· Evaluate BP and heart rate
· Evaluate renal arteries (renal artery imaging with duplex ultrasound, MRI/CT scan with contrast, etc.), if necessary as per local standards
· Evaluate renal function
· Note any adverse events
Further follow-ups will then be scheduled with your specialists to monitor progress following the procedure.
Is my procedure guaranteed to work?
It is essential to realise that from the published trial data that at least 10-20% of patients do not have a reduction in blood pressure following the procedure. There is no reliable way of predicting which patients may not respond to the RDN treatment, so your procedure cannot be 'guaranteed' to work.
Who will do my procedure?
A consultant experienced in intervention, who regularly undertakes the RDN procedures in their NHS practice, will do the procedure. There may on occasions be two consultants doing the procedure, although this will not affect the fee you pay.
Can I have RDN procedure done?
Following the recent release of a big trial in the USA (HTN-3) Renal Denervation has currently been suspended in the United Kingdom and is not currently available to NHS or self-funding patients, unless you are taking part in a trial. This position may well change in the future but for now we are unable to offer patients this procedure. Further information can be obtained by contacting Dr Wilkinson's secretary.
All patients will be assessed for suitability for this treatment and will need to undergo the following work-up prior to any treatment:
· A full consultation, including a full physical examination
· Evaluate Blood Pressure (BP) three times in clinic
· Have 24 hour ambulatory blood pressure monitor to demonstrate high blood pressure despite optimal treatment
· Evaluate kidney (renal) function
· Screen for diabetes
· Screen for other conditions that may prohibit renal denervation such as recent MI, pregnancy, etc. (Holter ECG, ambulatory BP monitoring, echocardiogram, cardiac MRI, NT-proBNP, etc.)
· Perform renal artery imaging with MRI scan
Once this work-up has been completed by a hypertension specialist, you may then be eligible for renal artery denervation. If you have secondary causes of hypertension, kidney failure or unsuitable renal arteries (assessed on MRI) then you cannot have the procedure. Your suitability for the procedure will be decided at a specialist MDT.
What happens after my procedure?
Following the procedure the following tests will be performed:
· Conduct a further physical examination
· Evaluate BP and heart rate
· Evaluate renal arteries (renal artery imaging with duplex ultrasound, MRI/CT scan with contrast, etc.), if necessary as per local standards
· Evaluate renal function
· Note any adverse events
Further follow-ups will then be scheduled with your specialists to monitor progress following the procedure.
Is my procedure guaranteed to work?
It is essential to realise that from the published trial data that at least 10-20% of patients do not have a reduction in blood pressure following the procedure. There is no reliable way of predicting which patients may not respond to the RDN treatment, so your procedure cannot be 'guaranteed' to work.
Who will do my procedure?
A consultant experienced in intervention, who regularly undertakes the RDN procedures in their NHS practice, will do the procedure. There may on occasions be two consultants doing the procedure, although this will not affect the fee you pay.
Can I have RDN procedure done?
Following the recent release of a big trial in the USA (HTN-3) Renal Denervation has currently been suspended in the United Kingdom and is not currently available to NHS or self-funding patients, unless you are taking part in a trial. This position may well change in the future but for now we are unable to offer patients this procedure. Further information can be obtained by contacting Dr Wilkinson's secretary.
Press coverage of RDN cases at Southampton

The first cases done at Southampton General Hospital attracted considerable media attention, which can be reviewed by clicking on any of the links below:
Daily echo article 1
Daily echo article 2
Daily echo video interview
ITV meridian coverage
Daily echo article 1
Daily echo article 2
Daily echo video interview
ITV meridian coverage